






















Topical Negative Pressure in Wound Care
Sylvie Hampton, MSc, RGN, Independent Wound Care Advisor
Introduction
Chronic wounds mainly affect the elderly and those with multiple health problems and despite the use of modern dressings, some of these wounds take a long time to heal, fail to heal, or recur, causing significant pain and discomfort to the person and cost to health services [1].
This delay in wound healing is a significant, particularly in older adults. In addition to the pain and suffering, failure of the wound to heal also imposes social and financial burdens. Topical Negative Pressure (TNP), also known as Negative Pressure Wound Therapy (NPWT) or vacuum assisted closure (VAC), has been developed as an alternative to the standard forms of wound management. It incorporates the use of negative pressure to optimise conditions for wound healing and requires fewer (often painful) dressing changes [2].
What is TNP?
TNP is a therapeutic technique used to promote healing in acute or chronic wounds, fight infection and enhance healing of burns and skin grafts. TNP is used to promote healing of chronic wounds and pressure ulcers by creating controlled negative pressure over the wound. The pressure is thought to:
- aid the drainage of excess fluid [1]
- reduce infection rates [1]
- increase localised blood flow increasing local vascularity and oxygenation of the wound bed
- reduce oedema through the increased blood flow and reduction of exudate and bacteria
This method seems to enhance the rapidity of wound reduction, and because it is a closed system of treatment, it has the added benefit of minimising exposure of staff and other patients to communicable diseases [3]. Thus, not only does TNP facilitate rapid granulation of wounds, it also reduces bacterial colonisation rates [4] .
TNP exerts a mechanical force on the tissues and attracts the wound edges centripetally while encouraging an increased peripheral blood flow, improved local oxygenation, promotion of angiogenesis, proliferation of good quality granulation tissueand removal of exudate through negative pressure [5,6]. However, there appears to be little evidence to support this and a review of TNP undertaken by Ubbink et al. [1] for the Cochrane Data base observed several methodological flaws in the execution of the different RCTs that they analysed.
Indications for use
The main limitation occurs of TNP is the maintenance of an airtight seal over irregular surfaces surrounding a wound. For example, application of the adhesive drape and creation of a seal are particularly difficulty in the hip and perineum. In addition, wounds of the lower extremity can occur in multiple sites, posing the problem of providing a vacuum dressing to more than one wound from one suction pump machine [7].
Nevertheless, the use of TNP has become widely accepted as adjunctive therapy for the treatment of non-infected, non-ischaemic diabetic foot wounds [8] and appropriate use of TNP can also achieve a rapid granular bed in diabetic foot wounds [9].
De-gloving injuries can be problematic to heal and numerous types of dressings have been devised but all are cumbersome and time-consuming, whereas TNP is an easy-to-use alternative to traditional methods [10].
A skin graft may fail to adhere to the recipient site because of fluid collecting between the graft and the area being treated. We have devised a simple procedure, consisting of a vacuum-sealed dressing, to fix skin grafts on the lower limbs [11].
TNP in pressure ulcer management
Although TNP can be useful for the above wounds, its starring position is in pressure ulcers where it can ensure a rapid healing with a reduction in infection potential.
The use of TNP can be as simple or as complicated as the person applying the dressing wishes to make it. TNP therapy consists of either a foam dressing or gauze dressing that is inserted into the wound and sealed in the wound by use of an adhesive dressing. Negative pressure is then applied by a machine which suctions out the wound fluid and debris through the foam or gauze and into a sealed container.
There are many manufacturers producing TNP products. Some are expensive and complicated to use so requires full training and consistent use of the product. Others are simpler to use and less costly. It depends very much on the formulary that is produced by the employing Trust or relies on the preference of the manager or the Tissue Viability Nurse. It is useful to know that many of the manufacturers will supply a pump free of charge if the dressings are ordered and charged.
There are now many TNP devices (see Figures 1 to 10). All have similar actions, different costs and often different applications.
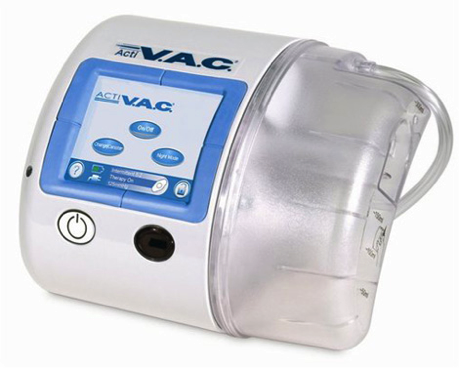



All of these and more designs can be found HERE
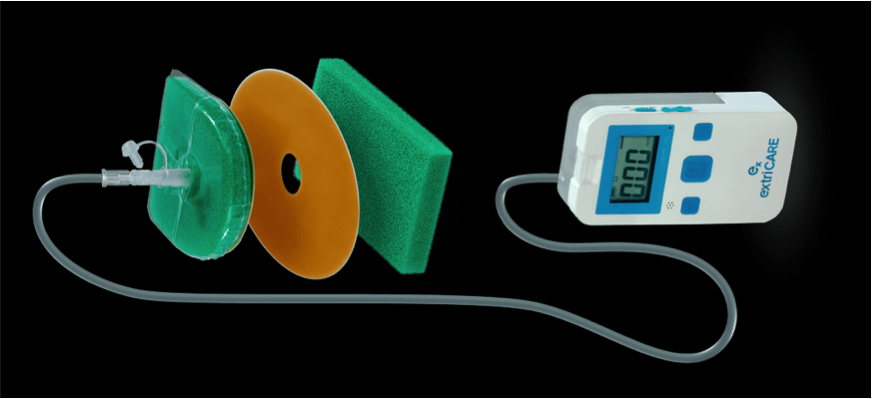
Figure 5.
Wound-Bag. Designed by nurses for ease of use. Found HERE
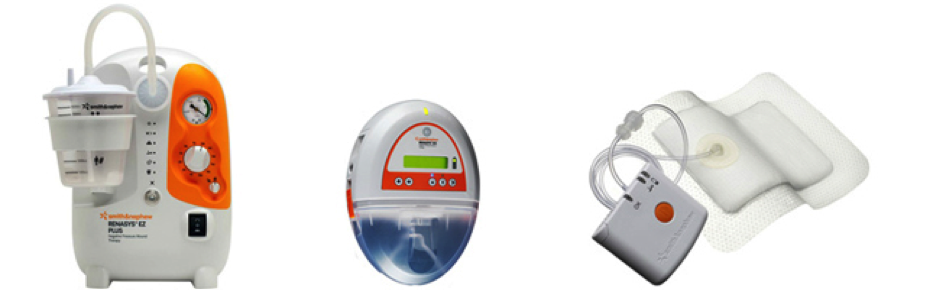
Figure 6.
A closed system, portable system and a simple dressing (PICO). All found HERE


Molnlycke products found HERE


Figure 10.
Found on many distributor websites.
Conclusion
TNP is an extremely valuable tool in the wound care box and amazing results can be achieved if used appropriately. If the correct device is ordered for the individual patient, then healing is simpler as there are less dressing changes and the patient experience is higher quality.